

Date: 27 February 2025 Time: 9:00 AM – 12:00 PM Location: East Coast Park NParks Office & KPMG Wellness Garden On a bright morning in late February, a group of 21 students gathered at the East Coast Park NParks Office for an insightful session on therapeutic garden design. Facilitated by NParks employees Afiq Fairuz (Landscape Architect and garden designer) and Dr. Agnieszka Olszewska-Guizzo, the Read More
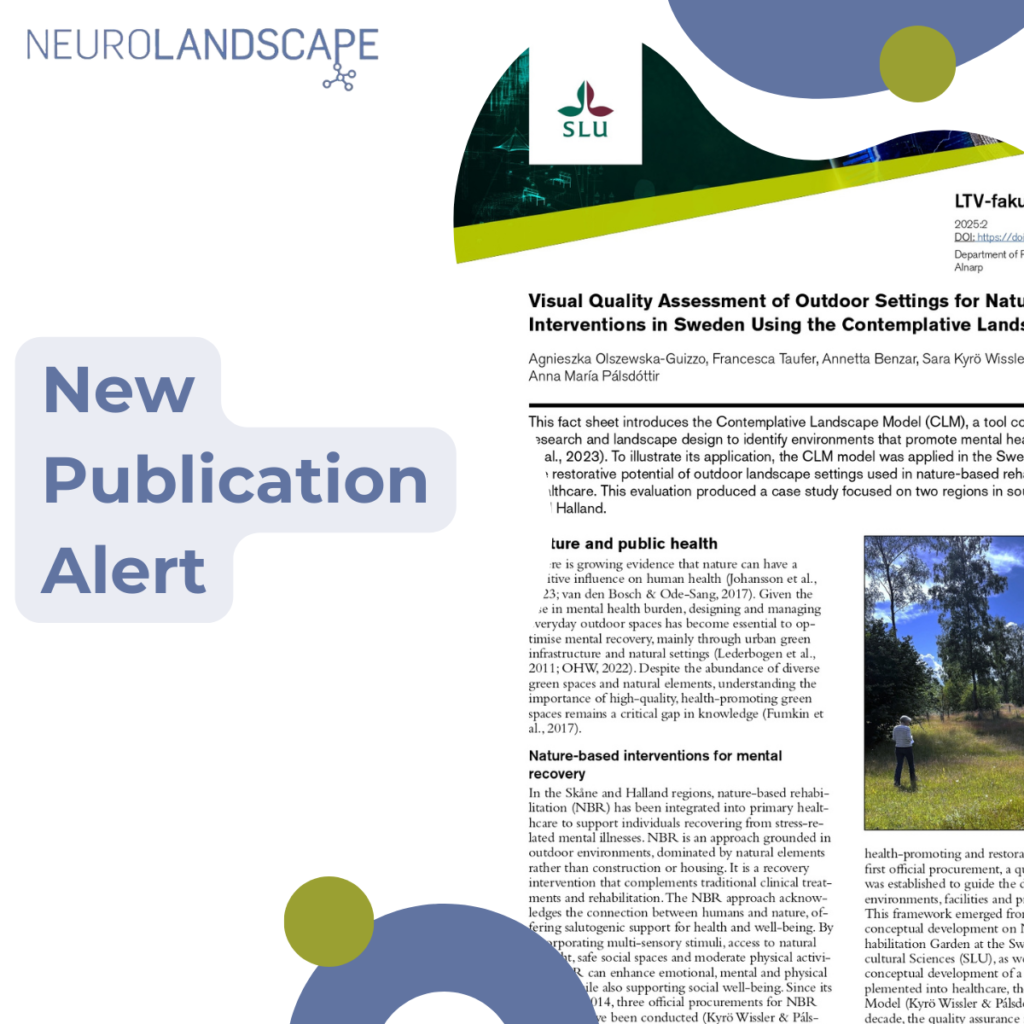
Category: Contemplative Landscape Model
Nature in Mind: An Interview with Erin Sharp-Newton
Erin Sharp-Newton, M. Arch, is the 2024 President for the American Institute of Architects Central New Jersey (AIACNJ.org) and serves as the Director of the Centre for Urban Design and Mental Health (UD/MH), founded by Dr. Layla McCay. She has been a Fellow of UD/MH since 2016 and holds the role of Section Editor of Read More

ICUH 2024: Green Care for Mental Health Equity and its Main Players
We are excited to share that our CEO, Dr. Agnieszka Olszewska-Guizzo, and our Gender Equality Officer, Dr. Weronika Gąsior, participated in the International Conference on Urban Health (ICUH2024) in Marrakesh, Morocco, to present the results from Work Package 2 of the GreenMe project. The conference, hosted by the International Society for Urban Health (ISUH), Read More

NeuroLandscape in Cork: GreenInCities Second Consortium Meeting
Cork, UK – October 8-9, 2024 Earlier this month, the NeuroLandscape team had the pleasure of attending the GreenInCities (GIC) Second Consortium Meeting in the vibrant city of Cork, Ireland. Hosted by the University College Cork (UCC) and Cork City Council, the two-day event gathered the international project partners to advance our shared mission: urban Read More

“A Talks” cycle ✨ Mental health – What does Architecture Have to do with it? ✨
5th November, at 19:00. National Art Gallery in Vilnius, Lithuania Our CEO Dr. Agnieszka Olszewska-Guizzo gave a talk titled “Can landscapes be healing?”at the National Gallery of Art in Vilnius. In this talk, Agnieszka explored the intersection between landscape architecture and neuroscience, which led to the creation of Contemplative Landscapes. She presented the science behind Read More

Designing for Well-Being: How the Contemplative Landscape Model Transforms Urban Spaces
We’ve all felt the calming effects of spending time in nature, whether it’s a stroll through a park or a quiet moment in a garden. But not all natural environments induce the same mental health benefits. Some landscape features, when combined, are more effective than others at promoting well-being, and the Contemplative Landscape Model (CLM) Read More
Nature in Mind: An Interview with Dr. Anna María Pálsdóttir
Dr. Anna María Pálsdóttir is the Senior Lecturer/Assistant Professor in Environmental Psychology at the Swedish University of Agricultural Sciences (SLU), the Department of People and Society. She is a professional horticulturist with a BSc in Biology & Horticulture Sciences and a MSc and PhD in Landscape Planning and Environmental Psychology. Dr. Pálsdóttir works with conceptual Read More

How Urban Design Can Impact Mental Health & Well-being
Our cities are often designed with function in mind. We build parks for exercise, wider sidewalks for pedestrians, and bike lanes for commuters. While we have made progress towards building healthier bodies, we have overlooked the equally important mental well-being. Urban design has a powerful influence on the quality of its citizens’ life, especially mental Read More

Building Back Differently: The Role of CLM in Public Health Promotion through Nature-based Solutions
“The future of humanity is undoubtedly urban,” warns the UN-Habitat in their World Cities Report (2022), urging public health policies to address the growing health risks associated with urban expansion. Urban environments — characterized by traffic, pollution, noise, and overcrowding — not only create fertile ground for physical health issues but also place a significant Read More